Joseph Lynch, MD
The Shoulder Clinic of Idaho
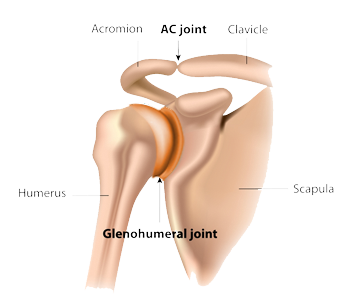
Rotator cuff tears occur by three mechanisms – 1) chronic tears associated with the natural aging of the tendon; 2) acute traumatic tears; and 3) acute-on-chronic tears. By far the most common reason for the rotator cuff tendon to tear is the natural aging process of the tendon – age related degeneration. Less common are the acute tears and acute-on-chronic tears. Among these two latter types of tears, dislocation of the shoulder joint is one of the more common mechanisms causing traumatic tears of the rotator cuff tendon.
For patients 40 years of age or older, a rotator cuff tear is a common injury resulting from a dislocated shoulder. Rotator cuff tears that occur acutely should be diagnosed early. For this reason, we recommend advanced imaging in all patients over the age of 40 who sustain a traumatic dislocation of their shoulder. An acutely torn rotator cuff tendon, in most instances, should be repaired timely. Much like a torn achilles tendon, torn quadriceps tendon, or torn distal biceps tendon; timely repair of an acutely torn rotator cuff tendon leads to the most favorable outcome in terms of improvement of a patient’s comfort and function.
How should your doctor identify a torn rotator cuff tendon associated with a dislocated shoulder? We recommend a MRI scan. We feel that an MRI is much better than CT and Ultrasound in the diagnosis of acute rotator cuff tears. This finding is supported by a recent study in the Journal of Shoulder and Elbow Surgery [1]. Authors from France, Australia, and Switzerland studied 67 patients who underwent arthroscopic repair of acute rotator cuff tendon tears associated with shoulder dislocation; and found that 12% of the tendon tears were massive rotator cuff tendon tears involving more than 2 of the 4 rotator cuff tendons without retraction. As a consequence of the absence of retraction (and reposition of the rotator cuff) several patients had false-negative ultrasound assessments. The authors recommended exhaustive radiographic assessment in patients whom rotator cuff tendon tears are suspected secondary to shoulder dislocation events, noting that non-displaced degloving tears may go unnoticed.
If you have sustained a dislocation of your shoulder and have persistent pain and/or weakness, or if you had difficulty raising your arm after your initial dislocation event; it is important to see a shoulder surgeon familiar with the diagnosis and management of acute tears of the rotator cuff tendon.
- Merlini L, et al. Hidden degloving rotator cuff tears secondary to glenohumeral dislocation. J Shoulder Elbow Surg. 2018;27:1456-1461.